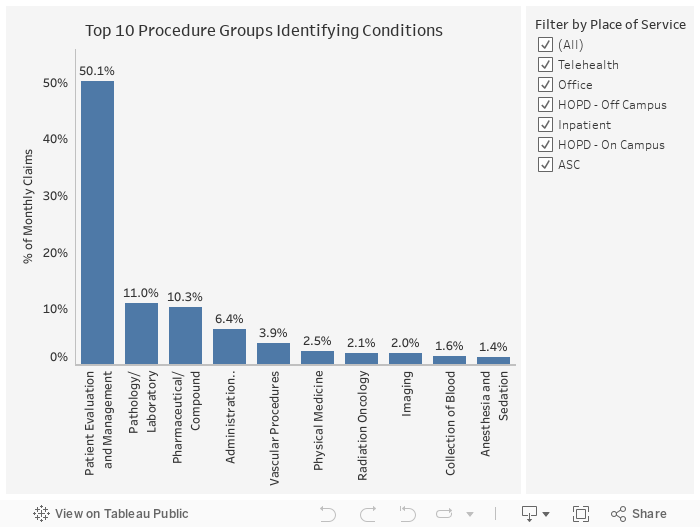
Using a proprietary dataset of 550K ACA lives from the Pareto Community, Pareto analyzed all scored claims with a documented HCC to identify the services, places of service and conditions that impact risk adjustment. This data has been updated through August 2020 and will continue to be updated as new data is available.
For the results presented below, the data is limited to scored claims from the places of service most impacted by COVID-19: Telemedicine, Office, Hospital Outpatient Department - Off Campus (HOPS-OFF CAMPUS), Hospital Outpatient Department - On Campus (HOPD-ON CAMPUS), Hospital - Inpatient (HSOP-INPATIENT) and Ambulatory Surgery Center (ASC).